 Français
Français4-year-old female with spontaneous XLH*
Case summary

Findings/outcomes
- Although the patient was seen by multiple specialists, a conclusive diagnosis was not reached over a period of 13 months, after referral to an endocrinologist; the patient was subsequently followed by a nephrologist
Although XLH is primarily an inherited disease, 20% to 30% of cases arise spontaneously.1
Patient history
18-19 months: Pediatric evaluation
- 18-month-old female presented with leg bowing, wide-based gait, delayed walking, and poor growth; fear of climbing stairs
- X-rays: indicative of metaphyseal dysplasia
- Other clinical findings: strabismus, suspected to contribute to walking delay; underwent strabismus surgery
28 months: Orthopedic evaluation
- Physical exam: short stature, height less than 5th percentile since age 15 months (See growth chart); worsened bowing and waddling gait
- X-rays: significant bilateral genu varum with mild beaking and sloping of the proximal tibial metaphysis; metaphyseal-diaphyseal angles of bilateral proximal tibiae measured 16 degrees; bilateral irregularity of the distal femoral metaphysis also noted; femoral heads were normally located
- Differential diagnosis: possible Blount’s disease, metaphyseal dysplasia, or physiologic genu varum
29 months: Genetics evaluation
- No family history of bone disease
- Suspected diagnosis: metaphyseal dysplasia
- Underwent genetic testing for Schmid metaphyseal chondrodysplasia and Shwachman-Diamond syndrome; results were negative for pathologic variants
- Diagnosis: unknown, referred to skeletal dysplasia clinic
31 months: Endocrinology evaluation
- Physical exam: bilateral genu varum
- X-rays: bilateral mild coxa vara, tibial varus (left greater than right) with metaphyseal irregularity and fraying of the distal femur, tibia, and ulna; metaphyseal widening at wrists
- Other findings: 2nd percentile for weight; 1st percentile for height (See growth chart)

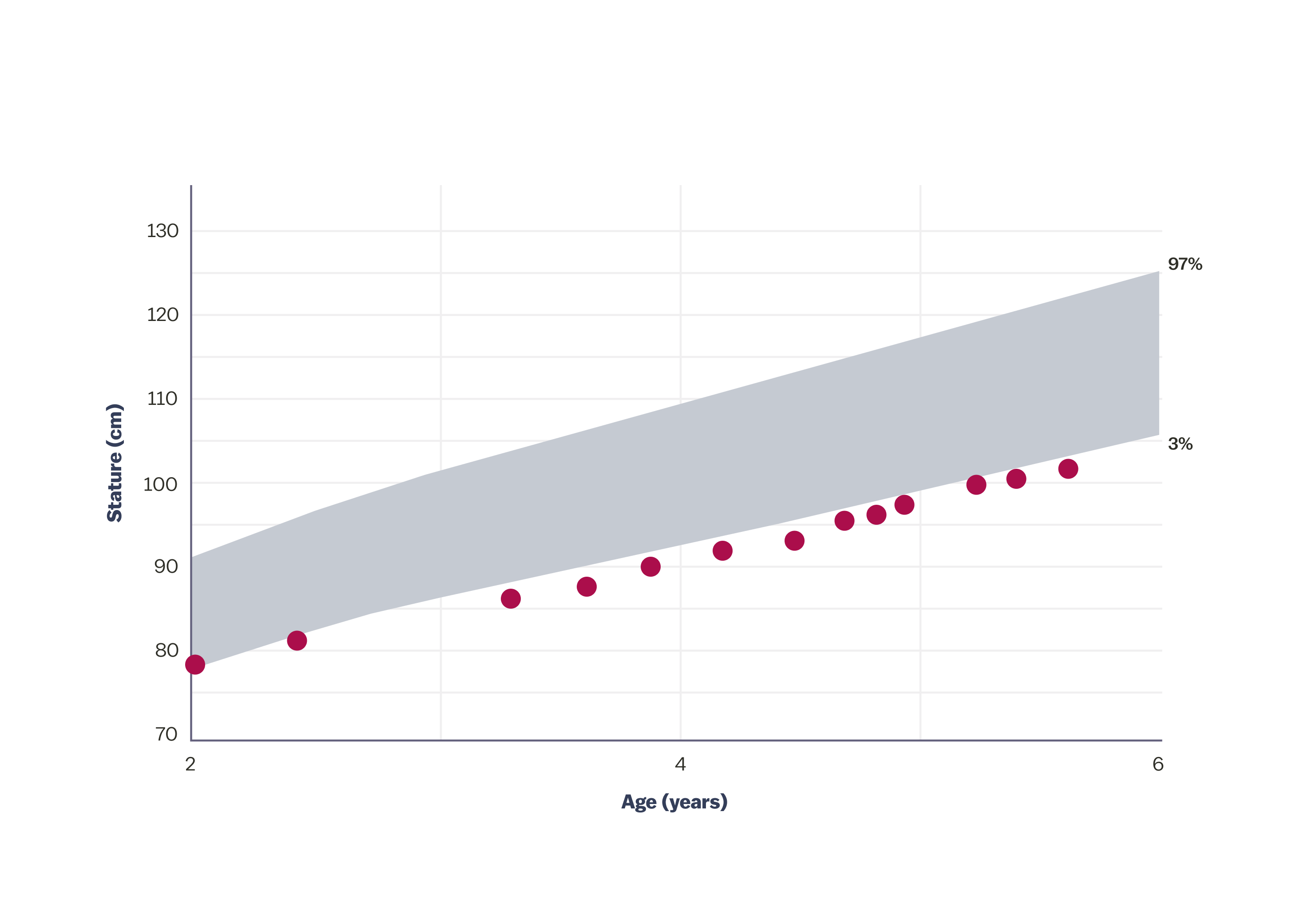
History of growth progression:
- Patient had short stature
- At 31 months, the patient was in the 1st percentile for height
Diagnosis
Hypophosphatemic rickets; positive for PHEX mutation; negative in parents—spontaneous X-linked hypophosphatemia
For patients with XLH, the diagnosis process can be long and laborious, and proper specialist referral can be key to early disease diagnosis.1,3
15-year-old female with spontaneous XLH*
Case summary

Findings/outcomes
- Bone health is an important consideration before growth plate closure
- Regardless of provider, asking about mental health was an important element of care
- Prevention of fractures and musculoskeletal health is critical
Symptoms of XLH are nonspecific when considered individually and vary between patients.1,3,4 Specialist referral is key to early diagnosis.
Patient history
- Birth: full-term infant with no abnormalities detected
- 12 months: signs consistent with pain upon weight bearing; limping; bowed legs at 18 months
- Family history: unremarkable
- 30 months: X-rays – bilateral bowing with irregular and widened metaphyses at tibia and femur
- 34 months: key fasting laboratory findings (reference range‡)
- Serum phosphorus: 2.4 mg/dL (3.2-6.1 mg/dL)
- 25-hydroxyvitamin D: 39 ng/mL (20-50 ng/mL)
- Alkaline phosphatase: 512 U/L (ULN for ages 1 to 15 years ranges from 297-385 U/L)
- Serum calcium: 9.2 mg/dL (0 to 2 years: 9.0-11 mg/dL; 2 to 16 years: 8.4-10.3 mg/dL)
- Parathyroid hormone: 85 pg/mL (14-72 pg/mL)

History of growth progression:
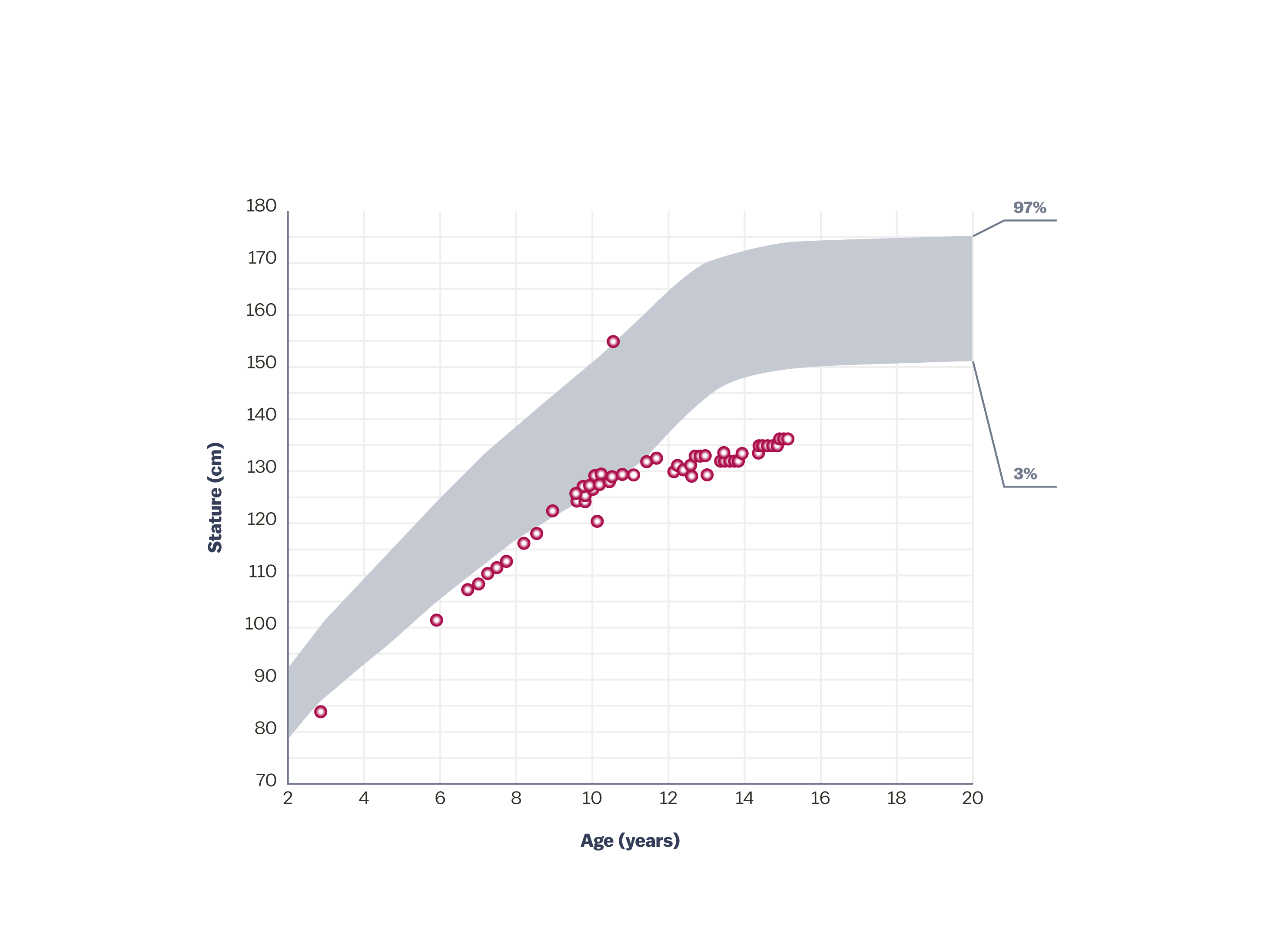
- Patient had short stature. Linear growth accelerated from 8 to 10 years of age, consistent with early growth spurt
Diagnosis
Spontaneous XLH
49-year-old male with hereditary XLH*
Case summary

Findings/outcomes
- The patient was not diagnosed with XLH until age 44
- There is a spectrum for XLH, and the patient’s symptoms were not previously attributed to XLH
- Symptoms of XLH progressed throughout adulthood and had long-term impact. The patient:
- Required surgeries and developed worsening pain
- Required the use of assistive walking devices
- Developed hearing loss
- Needed dentures
It is important to diagnose XLH early, as the progressive nature of XLH leaves patients susceptible to short stature, fractures, limited function, and pain.1
Patient history
During childhood
- 6 years of age: humerus fracture from jumping off a moving truck
- Poor dentition of both primary and secondary teeth with multiple cavities and abscesses
- 11 years of age: reported “bone disease” due to chronic bone and joint pain
- Pediatrician diagnosed post-streptococcal arthritis
- Mild leg bowing; reported short stature compared to peers
Early to mid-twenties
- Lost most teeth by early twenties
- Acute worsening of bone and joint pain
- Suspected inflammatory arthritis
44 years of age
- Presented with acute exacerbation of chronic weakness and right hip pain
- Reported no previous diagnosis of rickets
- Family history
- Short stature and bowing of the lower legs in mother (height, 4’11”), three brothers, and two nieces; all had multiple fractures
- Physical exam
- Height, 5’3”; weight, 230 lbs
- Ambulating with assistance of a walker; knees in varus alignment
- Pain with internal rotation of hips (left worse than right); 4/5 motor strength in both proximal and distal muscle groups
- Poor dentition and missing most secondary teeth
- X-rays
- Pelvis and hips: diffuse increased density of the bones, particularly in the iliac wings and lumbosacral spine; enthesopathic calcifications extending from the superior acetabular walls bilaterally (See X-ray 1); right subtrochanteric pseudofracture identified, which was incomplete along the medial cortical region (See X-ray 2)
- Femurs: pseudofractures in the subtrochanteric right femur and mid-left femoral diaphysis; healing stress fracture present in the medial cortex of the left femoral neck; enthesophytes and bilateral hip osteoporosis also noted (See X-ray 3)
- Laboratory findings (See Table)

44 years of age: Diffuse increased density of iliac wings and lumbosacral spine; bilateral enthesopathic calcifications extending from the superior acetabular walls.

44 years of age: Right subtrochanteric pseudofracture incomplete along the medial cortical region.

44 years of age: Pseudofractures in the subtrochanteric right femur and mid-left femoral diaphysis; healing stress fracture present in left femoral neck medial cortex; enthesophytes and bilateral hip osteoporosis.
Laboratory results
| Test (reference range unit‡) | 44 years (results) |
| Serum phosphorus (2.5-4.5 mg/dL) | 2.1 |
| 1,25(OH)2D (18-72 pg/mL) | 31 |
| 25(OH)D (20-50 ng/mL) | 33 |
| BSAP (6.5-20.1 mcg/L) | 39.2 |
| PTH (14-72 pg/mL) | 95 |
| Creatinine (0.7-1.2 mg/dL) | 0.83 |
| FGF23 (<180 RU/mL) |
73
|
The patient exhibited XLH signs and symptoms throughout childhood and young adulthood and was not diagnosed until his mid-40s.
Diagnosis
Hereditary XLH
Connect the symptoms
Suspect XLH?
Connect their symptoms and diagnose with the applicable tests.

The disease burden of XLH
Understand more about how XLH impacts the lives of patients.

XLH resources and community
Find resources for you and your patients to understand more about this rare condition.
1,25 (OH)2D=1,25 dihydroxy vitamin D; 25(OH)D=25-hydroxy vitamin D (calcifediol); BSAP=bone-specific alkaline phosphatase, also known as BAP; FGF23=fibroblast growth factor 23; PTH=parathyroid hormone.
* This case study represents a real patient and is intended to be illustrative. This case study does not claim to representative of the general population.
† The reference percentiles on the graph are combined from the 2 clinical growth charts for females 2-20 years of age provided by the Centers for Disease Control and Prevention.
‡ Indicates normal range, age, and sex matched. Note that normal range values may vary depending on reference dataset. Colored values are outside of the normal range provided by the physician and can raise suspicion of XLH.
References:
1. Dahir K, et al. J Endocr Soc. 2020;4(12):bvaa151. doi:10.1210/jendso/bvaa15. 2. Centers for Disease Control and Prevention. Clinical growth charts. 2 to 20 years: girls. Published May 30, 2000. Accessed May 21, 2019. https://www.cdc.gov/growthcharts/data/set2clinical/cj41c072.pdf 3. Hamilton AA, et al. J Endocr Soc. 2022;6(8):bvac086. 4. Haffner D, et al. Nat Rev Nephrol. 2019;15(7):435-455.